The goals of this clinical case are to discuss the different hypothesis and therapeutic options in case of a massive massive loss of bone stock around total hip arthroplasty.

- 57 years old gentleman
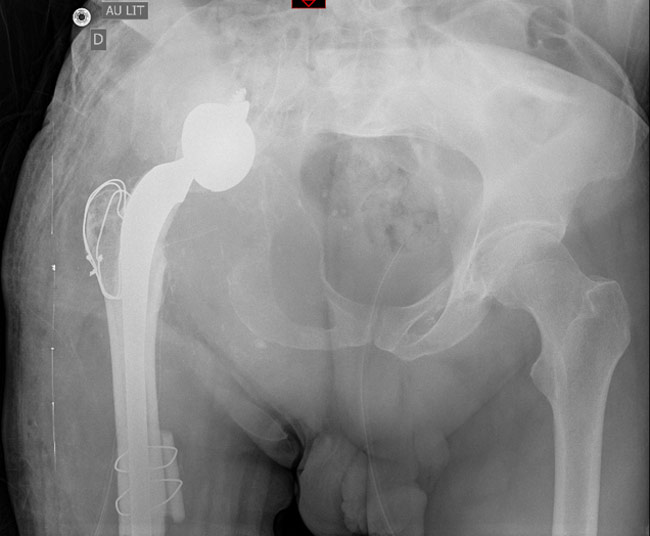
- Medical history: high blood pressure, right THR post-traumatic in 1993
- Right hip pain increasing for more than 10 years but patient was scared to see a specialist.
- Walk with 1 cane
- Lower Limb Discrepancy of 3cm
- Lateral and anterior incision on the hip not inflammatory
- Range Of Motion : 90 / 0 / 30 / 30 / 20 / 0
- Palpation of a soft mass in the groin
- Blood sample: normal hemogramm and CRP <5

What additional imaging or test do you ask?
- ✔️MRI
- ✔️Bone Gammagraphy
What are your diagnostic hypotheses?
- ✔️Metal allergy
Infection and cancer work-up were negative
A hip revision with a stemmed cup (transtrochanteric approach for gluts) and Allograft Prosthetic Composites was performed

A Lagrange and Letournel femoral cemented stem was implanted

Continuation of the patient's medical journey
At Post-Op day1, patient had increased pain, a sensation of instability and a sciatic nerve palsy (new)
A removal of the cup (in the sciatic nerve) was done

2 months after (without weight bearing and denutrition) a complex cup revision was performed

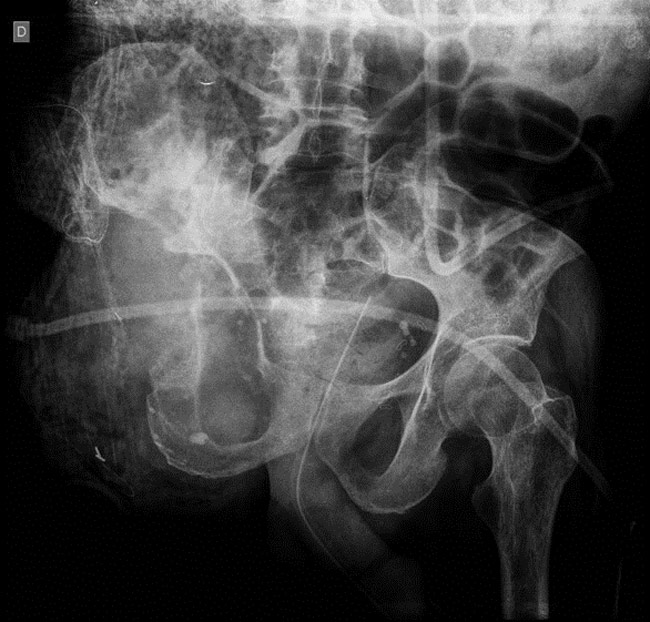
But... We noticed after removal of the drapes a massive knee instability that was not known before, and we asked for an x-ray.

Internal fixation was impossible because there wasn’t enough bone distally. A Hinge TKR and a bridging plate were fitted.

But it’s not finished…
- At Post-Op Day 12, hip and knee wounds were purulent, T°C was at 39°C and CRP at 300
- Patient underwent DAIR of hip + femur + knee
- At Post-Op Day 17 of the second surgery, CRP increased again at 250 (after having decreased), both wounds were inflammatory, T°C was 38°C (patient was under effective bi-antibiotherapy)
- A 2nd DAIR procedure was performed
- 2 weeks after, same septic failure happened and patient dislocated (several times)

A 2 stage surgery was planed: 1st stage of ilio-tibial spacer then total femur.
- During 1st stage, Blood loss were massive (15 red cells unit) and the patient was hemodynamicaly very unstable +++
- We Decided to close for hemostasis purpose before implantation of the spacer and decided a hip disarticulation after patient stabilised…

A Hip disarticulation was done one week later
Subscribe to our newsletter!
To receive the next clinical cases, subscribe to our newsletter!